Glue ear is a relatively common illness in childhood, also occurring in adults. It is one of the leading causes of hearing impairment in children.
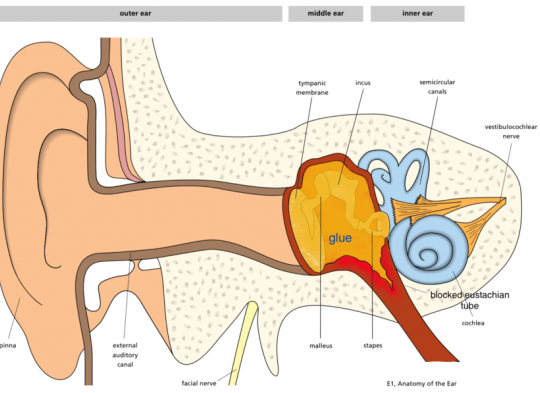
Glue ear is caused by the accumulation of fluid in the middle ear due to impaired patency of the auditory tube, most often resulting from hypertrophy of the pharyngeal tonsil. Other causes of fluid accumulation in the middle ear include upper respiratory infections, a history of acute otitis media, allergies, tumors of the nasal-pharyngeal region, scar tissue and fibrosis near the opening of the auditory tube (often as a result of radiotherapy), and pressure trauma, such as after a flight.
In adults, exudative otitis media, especially if unilateral, always requires thorough examination of the nasopharynx, as the cause of impaired tube patency could be a tumor blocking the opening.
Symptoms of glue ear include:
- Ear pain
- Conductive hearing loss
- A sensation of "fluid rushing" in the ear
The chronic form is characterized mainly by persistent conductive hearing loss (rarely mixed hearing loss) and sometimes tinnitus or dizziness. If the fluid persists in the middle ear for a prolonged period, some children may experience psychological issues, speech development delays, and difficulties in school.
Diagnosis of glue ear is based on otoscopic examination, which reveals:
- Honey-colored or yellowish tympanic membrane, sometimes with a visible fluid level behind the membrane and air bubbles
- Retracted and tense tympanic membrane
- Thickening of the eardrum with a tympanometric needle (vascular dilation along the handle of the malleus)
Audiology tests:
- Pure tone audiometry, which shows conductive hearing loss
- Tympanometry, which confirms immobility of the eardrum
- Acoustic reflex testing of the stapedial muscle—absence of reflexes indicates exudative otitis media
Treatment: After diagnosing glue ear, the initial approach is usually observation. Nearly half of children diagnosed with fluid in the middle ear experience spontaneous resolution. Scientific studies (conducted in the UK) and recommendations from the National Institute for Clinical Excellence (NICE) suggest that medication is ineffective.
If there is no improvement in hearing tests and tympanometry after about 3 months, surgical intervention is typically proposed—tympanocentesis (perforation of the eardrum) and insertion of ventilating tubes (grommets), which improve ventilation and allow drainage of the fluid. If adenoid hypertrophy is suspected, it is removed at the same time (adenoidectomy). Both procedures are performed under general anesthesia, and most children go home the same day.
All content on this website is the intellectual property of Poland Medical Clinic. Copying, reproduction, or dissemination in whole or in part, in any form or manner without the administrator’s permission, is prohibited; any unauthorized use will be considered a violation of copyright laws.


